
I Tried to Control My Blood Sugar With Exercise — It Didn't Work (At First)
The movement we lost without noticing
When we shifted to working from home, we lost something nobody really talked about: incidental movement.
Not exercise. Just movement.
The walk to a meeting room. Getting up to ask someone a question. Going to a kitchen on another floor. Even the commute—short or not—usually involved a bit of walking at either end. None of it counted for anything in your head, but it was there, scattered across the day.
I noticed it early in lockdown. Not in a dramatic way—more that whole stretches of the day passed without me standing up. Morning to early afternoon, barely moving. And by mid-afternoon, something felt off. Not just tired—flatter than usual, a bit foggy.
At first I assumed it was just the general shift in routine. But it didn't really go away.
So I started looking into it. Not exercise research—that's well covered—but what happens when you remove the small, frequent movement that used to sit around your day without you thinking about it.
That turned out to be more interesting than I expected.
Why this matters more than you think
Sitting for long periods (extended sedentary bouts) is associated with adverse cardiometabolic, musculoskeletal and cognitive outcomes. One area I found particularly interesting - the link to diabetes.
Most people don't think about blood sugar unless they have a reason to. It sits in the category of "medical things that happen to other people."
But the research has shifted quite a bit in the last decade.
Prolonged sedentary behaviour is now treated as an independent risk factor for type 2 diabetes, not just something associated with it. In other words, it contributes to risk even if you exercise regularly.
The numbers are uncomfortable. Each additional hour of daily sitting is associated with a meaningful increase in risk. People at the highest end of sedentary time have substantially higher relative risk than those at the lowest.
And this isn't about people who never exercise. There's increasing separation in the literature between what happens during exercise and what happens during the rest of the day. You can do the right things for 30–60 minutes and still spend most of your waking hours in a state that's working against you metabolically.
For remote workers, that's easy to do without noticing. The environment changed, and the prompts to move just… disappeared.
You can sit for hours now without anything interrupting you. No meetings in different rooms. No natural breaks. No reason to stand up unless you actively decide to.
So what is actually happening during those long stretches?
When you sit for long periods, your muscles become less effective at taking up glucose from the bloodstream. After meals, glucose rises more and stays elevated for longer. Your body compensates by releasing more insulin to bring it down.
That works—for a while.
But repeated over time, cells become less responsive to insulin. The body produces more to compensate. That's insulin resistance, and it sits upstream of type 2 diabetes.
This isn't a single tipping point. It's incremental. It's what happens during long, unbroken stretches of sitting, repeated day after day.
The useful part is that the mechanism also works in reverse. Movement helps. The question is how to apply that in a way that actually holds up in real life.
The principle everyone knows (but gets wrong)
The basic model is familiar. You eat, glucose rises, insulin brings it down.
Exercise helps—obviously. That part is well established and not up for debate.
Most people think about exercise as something you do once a day. A run in the morning, a gym session in the evening, something structured that you complete and then move on from.
For general health, that's a perfectly reasonable model.
For glucose, it's incomplete.
The gap that longer exercise doesn't fill
Regular exercise matters. Cardiovascular health, metabolic health, mental wellbeing—it's doing a lot of work.
But there's something it doesn't cover.
Short bouts of movement—two to five minutes—taken soon after eating can reduce the post-meal glucose spike. Not marginally; the effect is large enough to show up clearly in controlled studies.
The mechanism is fairly direct. Muscle contraction triggers glucose uptake via GLUT4 transporters, and that pathway doesn't rely on insulin. You move, muscles pull glucose out of the bloodstream more quickly.
Timing is the part that's easy to miss.
The glucose rise typically starts within 15–30 minutes after eating and peaks somewhere around 45–60 minutes. That window is where movement has the most impact. Earlier or later, and the effect is different.
Which means one session of exercise doesn't cover the day.
A morning run doesn't help with lunch. An evening walk doesn't affect breakfast. Each meal has its own window.
That's not how most of us think about it.
And it reframes something about office life that only became obvious in hindsight. A lot of the incidental movement we used to get—walking after meetings, getting up mid-morning, moving around after lunch—often landed inside those windows without us planning it.
It wasn't precise, but it wasn't random either.
Remove that, and you're left with long, uninterrupted stretches of sitting and no natural interruption points.
So I decided to test it myself
The idea was simple enough.
Wear a continuous glucose monitor (Abbott Lingo). Keep meals roughly consistent. On some days, add short movement sessions after eating. On others, don't. Compare what happens. To make it easier, I was only tracking/matching breakfast and lunch. After that, I was free to eat what I wanted, and I would not include data after 15:00.
I wasn't trying to do anything rigorous—just see the effect directly.
I had the CGM, an indoor bike wedged into my home office, and a couple of weeks where I could give it a decent attempt.
It should have been straightforward.
What actually happened
The glucose data itself was interesting straight away. Continuous, detailed—you can see the response to meals almost in real time.
CGM data from the first attempt, February 2026. You can clearly see the post-meal spikes. What you can't see is whether I moved, when, or how it mattered.
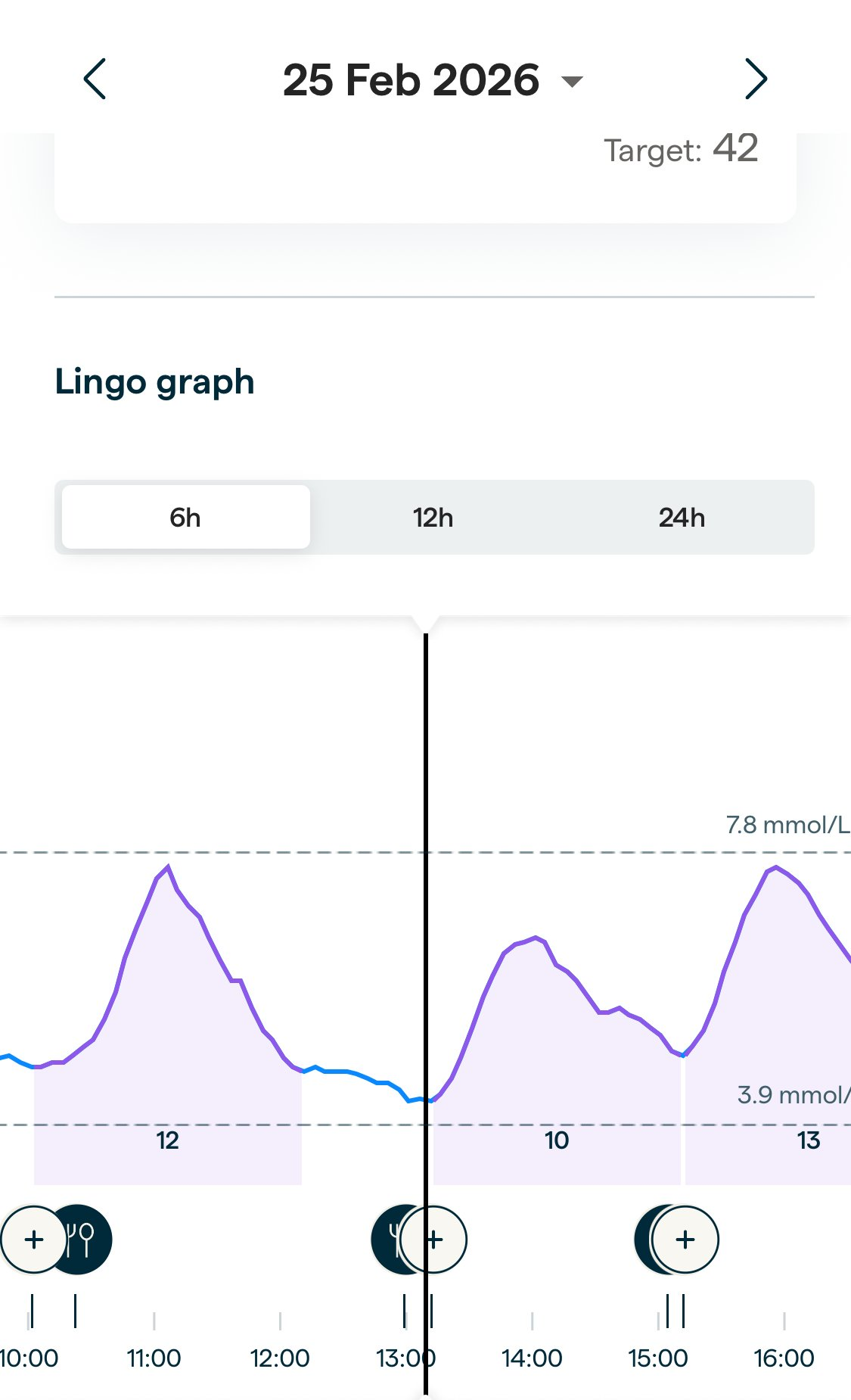
Example Day: Breakfast around 10:30, lunch around 13:00, snack around 15:00. Clear rises in glucose as expected. This was a non-control day - no intentional movement after mealtimes. Snack was a big snack: Toast + marmalade followed by a flapjack (I must have been hungry!)
But when I tried to turn the data into something comparable, it broke down.
The first issue was structure. I'd planned to alternate days—movement versus no movement—but within a few days that blurred. Some days I moved because it was "planned," others because I happened to think about it. Looking back, I couldn't cleanly separate them.
Activity logging was worse.
The things that mattered most were the easiest to miss—three minutes here, a short walk there. By the time I thought to record it, I was already guessing at the timing. And from a glucose perspective, that timing is the whole point.
"After lunch" isn't precise enough. Ten minutes after eating and forty minutes after eating are completely different interventions.
Even when I did log something, it was approximate.
Then life got in the way. I got shingles (first time, not nice!). Five days where eating patterns changed, activity dropped to almost nothing, and the experiment effectively paused. Eating patterns changed, activity dropped, and routine disappeared. Weekends didn't help either—different schedule, different food, less consistency.
I remember sitting at my desk one evening with the data open—CGM trace on one screen, notes on another—trying to piece together what had actually happened on each day.
It didn't hold together.
The outcome
The result wasn't negative.
I didn't show that movement has no effect. The underlying research is already clear on that.
What I had was a dataset I couldn't interpret with any confidence.
Different days looked different, but I couldn't reliably attribute why. Was it movement? Timing? Food variation? Something else entirely?
There was no clean comparison to make.
Which leaves you in an awkward position. You have data, but no clear signal.
The deeper problem
At that point it stopped being about glucose and started being about behaviour.
The intervention window is narrow. The timing matters. The actions are small and frequent. And the burden of tracking them accurately is high.
Even with motivation, context, and a deliberate attempt to do it properly, I couldn't sustain the level of precision needed to make sense of the data.
Not because it was difficult in isolation—but because it had to happen repeatedly, throughout a normal working day, alongside everything else.
That's where it breaks.
The advice itself—move after eating—is sound. But the way you'd have to implement it manually doesn't fit how people actually operate day to day.
If something depends on remembering, timing, and logging multiple small actions, every day, it's going to degrade. Not occasionally—systematically.
And usually at the exact moments where accuracy matters most.
What came next
So the next step wasn't trying to be more disciplined about it.
It was stepping back and changing the setup.
Remove as much manual input as possible. Let movement be detected automatically. Strip food logging down to something minimal. Define control and intervention periods in advance so you're not reconstructing them afterwards.
In other words, design the experiment around how behaviour actually works, not how you wish it worked.
That's what I'm setting up now.
A second attempt, with automatic movement detection, lightweight logging, and a structure that doesn't rely on memory.
I don't know what the data will show yet. That's the point. If the system is set up properly, it should be able to answer the question.
I'll share what happens.
I’m currently undertaking doctoral research in digital health, exploring how prompt-driven micro-movement interventions can offset the health effects of prolonged sedentary behaviour in remote and hybrid workers.The evidence linking sitting to metabolic and cardiovascular outcomes is strong. What's less clear is how to design interventions that actually work outside controlled settings.
This experiment—and the next one—is part of that.
If you want to follow along as the data comes in, subscribe below.
This research is informing what I'm building with Stirr, a platform and wearable for remote workers
The claims in this post are drawn from peer-reviewed research. If you want to check the evidence or read further:
Further reading
- Patterson et al. (2018) — Dose-response meta-analysis of sedentary behaviour and risk of all-cause mortality, cardiovascular mortality, cancer mortality, and incident type 2 diabetes. Covered 34 studies and over 1.3 million participants. European Journal of Sport Science / PubMed
- Wilmot et al. (2012) — Systematic review and meta-analysis of sedentary time and the association with diabetes, cardiovascular disease, and death. Found a 112% increase in relative risk of diabetes for the most sedentary compared with the least. 794,577 participants across 18 studies. Diabetologia / PubMed
- Dunstan et al. (2012) — Acute crossover trial showing that 2-minute walking breaks every 20 minutes significantly reduced post-meal glucose and insulin responses in overweight adults. Diabetes Care / PubMed
- Henson et al. (2016) — Breaking up sitting with standing or walking in postmenopausal women reduced the post-meal glucose rise by 28–34%. Diabetes Care
- Smith et al. (2024) — Systematic review and meta-analysis of interventions to reduce sedentary behaviour in adults with type 2 diabetes, finding significant improvements in glycaemic control. 28 studies included. PLOS ONE
- Latouche et al. (2016) — Skeletal muscle mechanisms underlying improved glucose control when prolonged sitting is interrupted with light or moderate walking. Showed contraction-mediated GLUT4 glucose uptake pathway is activated by brief movement bouts. Scientific Reports / Nature